Spotlight: Dr. Dung Nguyen
By Mohammed Al Kadhim
January 8, 2024
Dr. Dung Nguyen
Dr. Dung Nguyen is the Director of Breast Reconstruction and the Associate Director of Microsurgery in the Division of Plastic Surgery at Stanford Medicine. She has participated in numerous international teaching and medical mission trips. We caught up with her to discuss her career and experience.
Tell us about your training and clinical background.
I’m a plastic and reconstructive microsurgeon. I did my plastic surgery residency at Los Angeles General Medical Center (LAC+USC) where I was exposed to a myriad of complex reconstructive surgery techniques. I was drawn to the technical challenges of microsurgery and was inspired by the transformative nature of these operations. We can take a patient with a congenital facial deformity, a mangled extremity from trauma, or a big open wound in the abdomen and transfer healthy tissues to restore form and function and give the patient a new life. I love that we are giving people hope with surgery.
After residency, I did a microsurgery fellowship at Chang Gung Memorial Hospital in Taiwan. At that time, it was considered to be the largest reconstructive microsurgery center in the world, with over 1000 free flaps performed each year. My fellowship was an important part in my training because it exposed me to leaders and pioneers in the field who shaped the evolution of my career. At Chang Gung Memorial Hospital, I worked side-by-side with some of the giants of microsurgery like Professors Fu-Chan Wei, David Chuang and Ming-Huei Cheng who introduced me to tissue transplantation, peripheral nerve reconstruction and lymphatic surgery.
You have served as the Director of Breast Reconstruction at Stanford Women's Cancer Center for over a decade. Tell us about the advancements in this field and some of the remarkable landmarks you and your team have achieved and witnessed.
My practice at Stanford in the last decade has been primarily focused on breast reconstruction and lymphedema, and I have been heavily involved in the clinical and research aspects of both those fields. Our breast reconstructive service has significantly expanded both in volume and types of services, and we now offer a full spectrum of reconstructive options for patient who undergo mastectomies and lumpectomies. We have created reconstructive solutions for some of the most challenging patients that have been deemed poor surgical candidates elsewhere.
We have refined techniques for nerve-sparing mastectomy, developed new approaches to re-innervate the nipple and flap to improve sensation after mastectomy and reconstruction. We have developed a variety of new breast reconstruction techniques like combining flaps with implants, and the technique of omental flap reconstruction. Our breast team has also developed ways to preserve perfusion to the nipple complex which allows us to do nipple-sparing mastectomy even in irradiated and diabetic patients which historically has not been possible. Here at Stanford, every patient can be offered nipple-sparing mastectomy if there is not an oncological restriction.
In addition, we now have options to treat and prevent lymphedema. We have developed a comprehensive Surgical Lymphedema Program at the Women’s Cancer Center and established a multimodality treatment algorithm that slows the progression of lymphedema and can normalize a patient’s limb volume. We also established a new service for lymphedema prevention that involves axillary reverse mapping and immediate lymphatic reconstruction at the time of axillary lymph node dissection.
All these new techniques and services that we have added allowed us to provide comprehensive treatment to patients who have gone through breast cancer treatment. We have patients regionally, from other states, and overseas who come to Stanford specifically for these reconstructive options.
 – NBC News
– NBC NewsBreast cancer reconstruction procedure offers an alternative to usual methods
On the last day of Breast Cancer Awareness Month, NBC's Vicky Nguyen speaks with a doctor at Stanford Women's Cancer Center on a little-known breast cancer reconstruction procedure involving Omentum to create a breast implant out of a person's own body tissue.
You’ve pioneered the work in omentum breast reconstruction. Tell us about this technique: when did it start and what benefit does it bring to breast cancer patients who have undergone mastectomy?
This technique was developed to address an unmet need in breast reconstruction, especially for thin women as an alternative for tissue-based reconstruction. Historically, these patients had only one option which was implant-based reconstruction. Recently, there are more patients seeking omentum breast reconstruction who do not meet the standard criteria for traditional autologous reconstruction and who don’t want an implant reconstruction due to concerns for anaplastic large cell lymphoma and breast implant associated illness.
The innovation came about four years ago through my interaction with a patient and one of our breast surgical oncology colleagues, Dr. Irene Wapnir. That patient was a nurse who is very slim and very physically active. She had a prior history of breast cancer treatment and now had a new cancer, but she really didn’t want to have an implant-based reconstruction and was looking for an alternative option. This request started us in a discussion on what else can we offer, and we contemplated using the omentum.
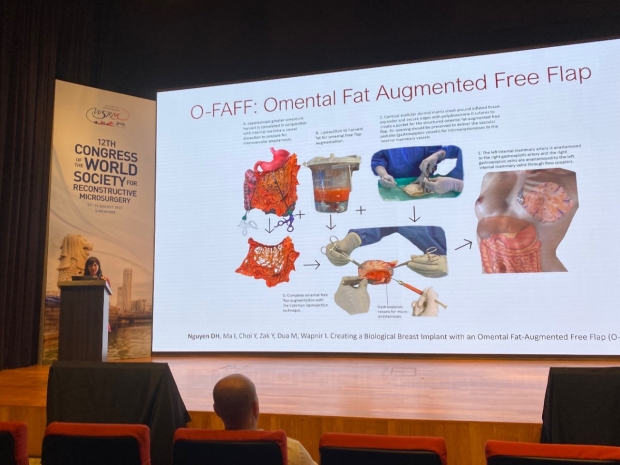
The omentum is a sheet of tissue that’s flat, it contains fat, blood vessels and lymphatics. The omentum has previously been used in breast reconstruction in the early 20th century. However, its use has been limited to pedicled reconstructions where the blood supply is kept attached to the stomach. It is brought out of the abdomen and simply sutured to the chest wall. This results in a flattened contour and an abdominal hernia at the donor site. There is also more pain and post-op complications associated with an open harvest. The challenge for us was to create something that has shape, volume and projection using this sheet of tissue. The innovation comes from combining principles that we are already applying for breast reconstruction in a novel way to create something new.
Essentially, we’re creating an implant from tissue by using a biological mesh to create a pocket to hold the omentum and the fat. The omentum, which is harvested laparoscopically by our laparoscopic surgeons, provides the volume, and serves as a vascular flap to increase fat viability. We then inject the patient’s fat into this flap to give it additional volume. The blood vessels to the omentum are reconnected with microsurgery to bring blood supply to the entire reconstruction. So here, we apply the principles of free tissue transfer, fat grafting, and soft tissue reinforcement with a biological mesh to create shape and volume.
The key advantages we found with this technique are quicker recovery time, shorter hospital stay, less post-operative pain, and smaller scars. So, in fact, the patient is getting a natural reconstruction without having the traditional downsides of using her own tissue.
Earlier this year, you and Dr. Irene Wapnir received the Stanford Cancer Institute Innovation Award for your proposal on “Volume and Symmetry Outcomes in Unilateral Omentum-Based Breast Reconstruction.” Tell us about this work.
This grant allows us to study our results in patients who have a unilateral omentum breast reconstruction. It allows us to analyze the postoperative volume and symmetry using MRI. The main limitation of the omentum reconstruction is the inability to predict how much omentum a patient has preoperatively. Also, there isn’t an accurate way to assess the degree of fat retention after engraftment. This study will allow us to evaluate this more objectively. This would in turn allow us to optimize the breast reconstruction and better predict the size limit that we can create with the omentum.


You are also known for your medical mission work and your participation in medical charity activities. How would you compare the microsurgery techniques that are practiced in the US with those in other countries that you had visited?
Microsurgery techniques, in my opinion, are universal. Since the first development of the microscope in the 1950s, there have been advances in the field of microsurgery in terms of better and finer instruments, smaller sutures, and higher magnification.
As I travel around the world and visit different microsurgery centers, I have noticed subtle differences in the equipment that are available and used for microsurgery. Some of it is reflected by the resources that are available. For example, some surgeons in Asia where microscopes aren’t available use loupes to do surgery. In Japan where there is access to much finer instruments, super-microsurgery is commonly performed commonly. In the US, vein couplers are commonly used for the vein anastomosis while most Asian and some European countries still handsewn the veins because they don’t have access to vein couplers.
Although instruments and technology can enhance the technical experience, the fundamental microsurgical principles, and techniques such as suturing, knot tying, and flap monitoring are pretty universal. That is why we can do microsurgery anywhere in the world, even with basic instruments.
What have been the most valuable lessons and experiences on your trips?
Medical volunteerism is a way for me give back to the community. My experiences have been both humbling and inspiring at the same time. One of the most enjoyable parts of being on a mission is having the opportunity to learn about another country, its people, and its culture. Through collaboration, we overcome our biases, learn to be resourceful, and conquer challenges to create the best team dynamics possible for a successful mission.
The patients’ stories are often unforgettable. It is heartwarming every time I hear a story about how a patient’s life was transformed for the better because of our effort. This will never get old for me.
The most valuable lesson I learned through my medical missions is the importance and power of organized effort for scalable impact. As a single surgeon, I can help 10-14 patients per trip. As a team, we can empower surgeons through training and mentorship so that they can help hundred and thousands of patients in the long run. Through partnerships with non-profit organizations like ReSurge International, we can leverage infrastructure and organizational capabilities to achieve scalable lasting impact.
You have hosted many international visiting observers in your division. How would you assess the outcomes and learning benefits gained by the visitors? And how can the Global Engagement program at Stanford Surgery help to build more educational bridges and global bidirectional partnerships?
Global Engagement represents bidirectional partnerships. It’s an honor to have visitors from around the world come to Stanford to observe and learn what we do. At the same time, it creates opportunity for academic exchange and collaboration. In the past year, we have had more than 10 visitors from Canada, Asia, and Europe. Now with social media and the internet, we can maintain connection with colleagues simultaneously in different countries. Global partnerships are becoming more like a multi-directional collaborative network that we can continually draw from.
What is most rewarding for me is getting feedback from the visitors after they return to their home program and hearing how they applied what they have seen and learned during their visit to treat their own patients. Some of them have developed new programs as a result or developed research ideas that lead to collaborative projects.
You recently completed the James IV Travelling Fellowship. Tell us about this.
The James IV Travelling Fellowship is a great example of a mechanism for global engagement. I recently completed the ![]() James IV Association of Surgeons Traveling Fellow in 2022-2023. This award is given to US, UK, and Canadian surgeons, and allows the awardee an opportunity to travel around the world for academic exchange and collaboration. I was able to visit different centers in Canada, Europe, and Asia to learn what they do and as well as share what we do for breast reconstruction and lymphedema treatment. Through those connections I now have new opportunities for research and have developed new friendships.
James IV Association of Surgeons Traveling Fellow in 2022-2023. This award is given to US, UK, and Canadian surgeons, and allows the awardee an opportunity to travel around the world for academic exchange and collaboration. I was able to visit different centers in Canada, Europe, and Asia to learn what they do and as well as share what we do for breast reconstruction and lymphedema treatment. Through those connections I now have new opportunities for research and have developed new friendships.
James IV Travelling Fellowship is sponsored by the James IV Association of Surgeons which is a prestigious organization of 100 members from around the world who are internationally renowned and are surgical leaders in their own country. Dr. Tom Krummel was a James IV Traveler and Dr. Mary Hawn is on the Board of Directors. Candidates for the Travelling Fellowship are nominated by the department chair or a James IV member. The nominee then applies, indicating their goals for the fellowship, where they want to visit, and what they want to learn from their trips. The applicant nominations are reviewed and voted on by the Board of Directors. Nominees are selected based on their academic achievements and potential as emerging leaders in surgery.
Thank you for sharing your journey with us! Can you tell us a few personal milestones that you are most proud of?
I am proud of my contributions to research and clinical practice that have advanced and improved patient outcomes. I am also very proud of helping grow and develop the microsurgery program over the past 11 years. My biggest personal achievement at Stanford University was my promotion to full professor after nine years. This year, I assume the role of the Director of Microsurgery and Fellowship Program. This is another huge personal achievement for me because it is a specialty that I’m very passionate about. I love teaching and being in a position where I can lead and be a mentor for future fellows and young microsurgeons is extremely rewarding for me.