Stanford Fellow Volunteers in COVID-stricken New York City
May 27, 2020

Daniel Peyser, MD (PGY2-3) was 1 of the 4 research residents (Schmiederer included) who came back to clinical duties to help at NYPQ

Schmiederer takes a selfi to show off the impressions left by her N95 mask.

Schmiederer flew out April 8th and was in full ICU senior resident mode by April 12th.
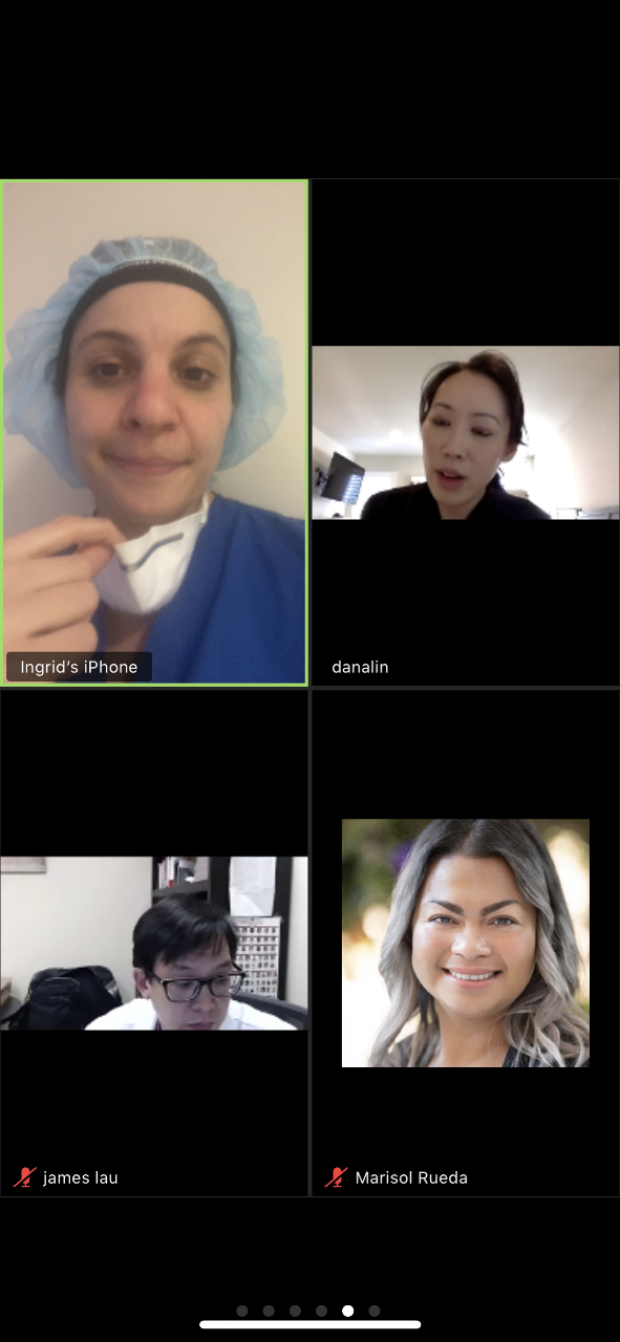
Schmiederer attends a virtual GSEC team meeting while on a break in the hallway at NYPQ.

Schmeiderer would don a 3M suit with her name written on the back in permanent marker.
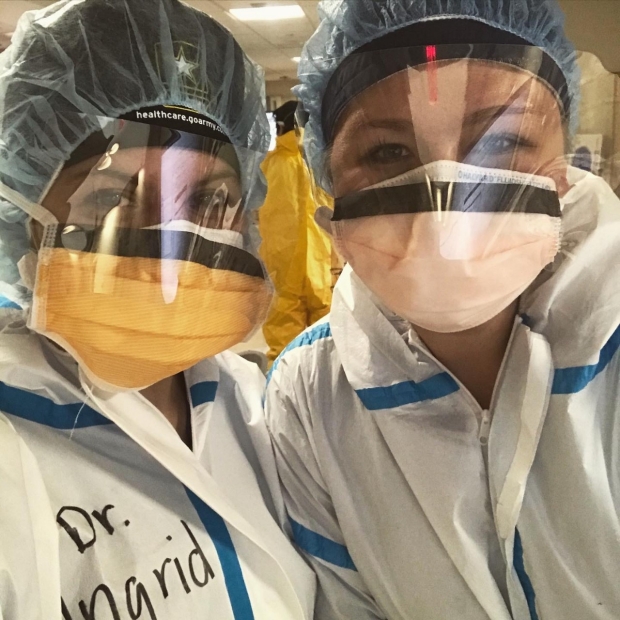
Teagan Thorson, DO, a current PGY3 at NYPQ and Schmiederer take a quick “birthday selfie” during a COVID ICU shift. Thorson is a current PGY3 NYPQ surgical resident who started working in the COVID ICUs in mid-March.
On April 8th, Dr. Ingrid Schmiederer boarded a flight from SFO to LGA. She was electively charging into what was then the epicenter for novel coronavirus cases in the United States and the world. As a Surgical Education Fellow, Schmiederer could have stayed on the sidelines of the pandemic. Instead, she volunteered for five weeks at her home hospital, NewYork-Presbyterian Queens(NYPQ).
Rachel Baker: Why go back?
Ingrid Schmiederer: In early March, there were three patients in the medical intensive care unit (MICU) at NYPQ. By the end of March, the hospital was maximizing 535 beds to accommodate upwards of 600 COVID-only patients—even the hospital cafeteria was converted to a COVID unit. 200 of these patients needed ICU-level care.
Residents, PAs and attendings from the surgery department all joined the effort within the hospital and managed four of the seven ICUs, as well as the line team, the proning team, family ambassadors and food runners. Much of the ICU resident work was taken on by my friends in the PGY3 class. There were few to no surgeries—just medical ICU COVID patients.
It didn’t seem right for me to be working from home on my quiet couch in California, while my friends were coding patients every few hours and taking on more shifts to accommodate the growing number of patients with short staffing, nursing, supplies, etc. They were more than capable and resilient enough to rise to the challenge and continue that way, but I wanted to support them in any way that I could.
It made the most sense for me to come back to NYC. I ended up working about 25 of those COVID ICU shifts while I was in Queens. It allowed for my friends to take on fewer patients and have a few extra days off to rest.
RB: What was a day like?
IS: My day started between 6:30 and 6:45 a.m., when I arrived at the hospital, wearing street clothes and a regular surgical mask (or a cloth mask donated to hospital workers by local volunteers). I changed into my scrubs in the PGY3 call room and then put on my N95 mask, a surgical scrub cap, and a surgical mask over the N95 to keep it clean as long as possible. From the 8th floor call room, I took the stairs to the 2nd floor ICU, which used to be the cardiac cath lab recovery area.
Outside of the resident work area, I kept a Tyvek or 3M suit with my name Sharpied on it. I would put gloves on first and then don my suit. Then a second layer of gloves. After that, I would tape a specimen plastic baggie around my phone and place my phone in my makeshift pocket (another plastic baggie taped to my suit pantleg like cargo pants). By 7 a.m., I would receive sign-out from the night team and plan to round with an attending by 8 a.m. The shift lasted until 7 p.m. when I would sign out to the night team again.
The hours were actually better than standard surgical duty hours. We worked four or five 12-hour shifts with two days off in-between. The issue was really the emotional and physical toll of the ICU for those shifts. The first week I was there, nursing was short staffed, so I actually learned a lot from my favorite Surgical ICU nurses about nursing tasks, like hanging drips, turning patients, titrating medication, blood draws, IVs, etc.—fruitful experiences, albeit exhausting.
In that same week, I also found myself losing about one or two patients per day, with a new patient coming into the same ICU spot two hours after the deceased patient was cared for and moved to a different area of the hospital. Using Facetime and phone calls to update families or allow for them to say their final goodbyes took its emotional toll.
There was another week where I was doing CPR about once or twice a day. It was a physical and emotional workout inside that sweaty suit. These patients could crash at any moment despite our best efforts. Everyone I treated was already intubated and nearly half were already in renal failure on dialysis. It was a mental struggle to come to work every day unsure of which patients would still be on the list and which of our efforts proved futile. I found myself overly protective of patients I had been treating for weeks and witnessed progress and even more emotionally invested in patients who were closer and closer to my own age.
At the end of my shift I’d go “home” to my hotel room and sleep or attend virtual counseling sessions provided by the hospital before coming back to work the next day. My Residency Program Director, Dr. Chris Foglia, kept resident wellness as a priority, despite the circumstances. It definitely fostered great comradery among the surgery residents at my program.
RB: You mentioned learning from SICU nurses and building a special bond with your fellow residents. Were there other silver linings?
IS: The attendings changed weekly and were honestly one of the best experiences. My first week, I rounded with NYPQ surgical and medical intensivists. The second week was with two intensivists volunteering from Cleveland Clinic: Drs. Kar-Min Lo and Pravin George. The third week I rounded with Dr. Rebecca Plevin, who flew in from Trauma-Critical Care Surgery at UCSF. The experience with diverse approaches and personalities was invaluable. I would not have experienced this level of education from so many different attendings anywhere (or anytime) else.
RB: What happened with your fellowship?
IS: Dr. [James] Lau, who is also a former member of the military, absolutely understood my need to serve so he generously and patiently let me go back to NYC and try to work remotely on Stanford work between shifts as much as possible. Mostly, our Zoom meetings became mental health check-ins and wellbeing breaks, for which I am really grateful.
RB: How do you think this experience will shape your future in medicine?
IS: My friends at NYPQ and I talked a lot about this. Many of them are native New Yorkers/East coasters. I think this feels like what September 11th must have felt like for the first responders at that time. There is a level of trauma associated with this experience, but also a feeling of resiliency and pride in being in healthcare at this historic time. I absolutely think this has positively impacted my personal confidence as a physician but also as an educator. We survived this insane challenge; we can handle the rest of surgery residency and beyond.